
Use the Search magnifying glass above to search the site. Use CNTL+F to find text on pages; Apple, use Command+F.
The Mask - A Working Hypothesis

COHERENCE, Vol 1, Issue 2 , December 23, 2021, by Stephen Elliott, Life Scientist, COHERENCE
This article was updated on February 11th detailing my experience with what I think was Omicron.
Article posted on CNN.com on December 24th, 2021.
We’re all being implored by the CDC to mask-up, especially when in in-door crowded spaces. My personal observation is that many observed this “masking protocol” during the COVID Alpha-wave (2020 timeframe), after which concern/compliance by the general public began to wane. Now most of the mask wearing I see is by those serving the public, either wearing masks or operating behind clear barriers or both, this during the Delta-wave dominating most of 2021, even as case counts surged, filling hospitals, and picking off friends and loved ones. A tragedy of immense proportions.
Please understand that I live and work in north Texas, a deeply red state where mask wearing has been highly politicized and mask mandates are being challenged by state government- where mask mandates by federal agencies and or government are argued as an assault on personal freedom. Note that the Texas legislature recently passed into law the right for every adult age 21 and over, to carry a firearm on their person without without a license, i.e. without prerequisite training and demonstration that one understands how to handle a weapon before being allowed to carry one in public. This went into effect in September of 2021. One might easily develop the impression that here in Texas “personal freedom” outweighs public safety. But then there is the matter of a woman’s right to abortion…
However, there is a real stumbling block in the mind of the public regarding mask wearing, this being “doubt” about the effectiveness of a mask in preventing the transmission of disease, specifically COVID-19. Here in Texas, this doubt is reinforced by the action of the state government, especially in the minds of those that are politically aligned with state governmental policy. At the same time, many of the strongest voices for compliance with CDC protocols are those of MDs and virologists at leading hospitals and research universities here in Texas, including some of the nations most respected medical schools. So you see, we have a real “wedge” problem here in the 2nd largest state as in many other red states where state policy makers are at odds with federal recommendations, specifically regarding COVID mandates. I chalk it up to political theater, but theater that comes at a very high price: illness, disease, and death, with consequences both short and long term. We’re about to find out if or how Omicron changes behaviors…
~
Update
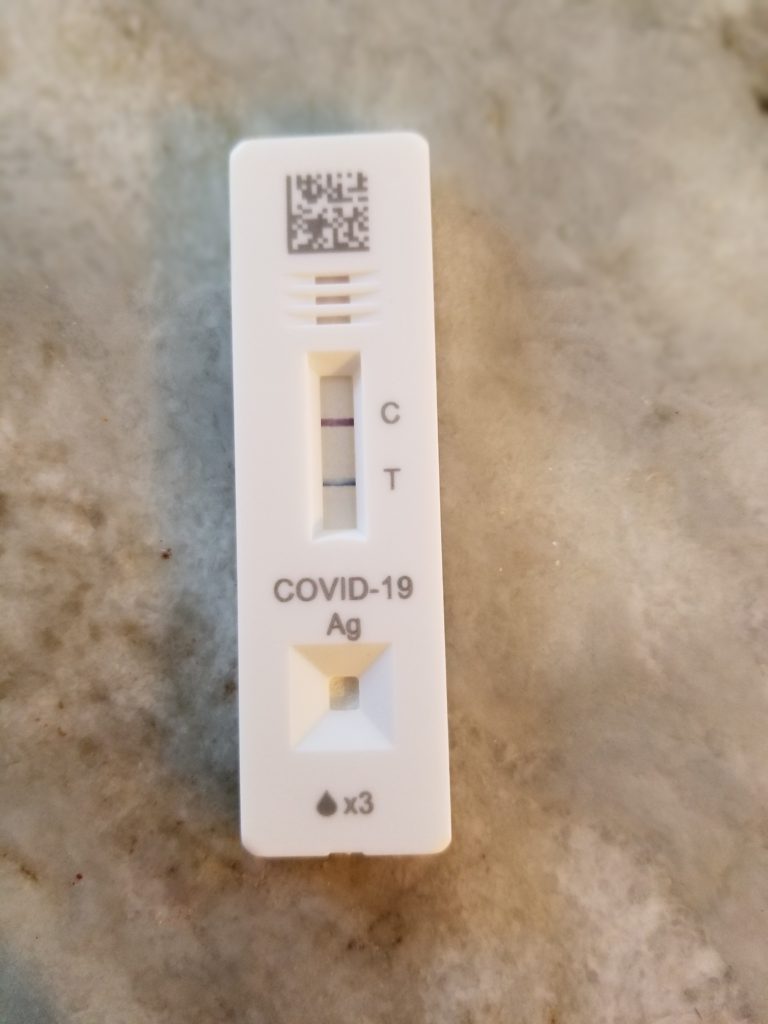
A Positive COVID Test Outcome
Sometime before January 23rd, I myself contracted COVID – what I suspect was Omicron. I tested positive on the 23rd after experiencing a runny nose with a spot of blood here and there, apparently coming from my sinuses. I believe I know when and where I came in close contact with it, which was about 2 weeks before these symptoms began. However, at this time I had no other symptoms that would even suggest that I had a cold. Here, I mean no headache, no sinus discomfort, nothing that would suggest that I had contracted Omicron. (My observation is that Omicron, in keeping with findings about COVID-19 in general, infects one but without any tell-tale feelings that one is ill, i.e. “stealth mode” at work.)
I quarantined for 5 days and stayed on my normal health regimen, making sure that I wasn’t forgetting to breathe with depth and rhythmicity which appears to be part of COVID’s stealth modus operandi. About a week into this phase, I could feel irritation starting to creep down my pharynx and into my upper chest. Given that I’d tested positive I was hitting it with everything I have, but to this I added 10 minutes on a nebulizer, twice per day with 1 drop of colloidal silver, 1 drop of food grade iodine, in a tablespoon of saline solution. This helped immediately, both clearing my sinuses and alleviating signs of it moving toward my lungs.
Otherwise, I felt a bit like I had the flu but only now and then. Here I mean that I would feel achy and then the achiness would vanish completely, and then it would return in the afternoon, common timing with the flu and respiratory bugs. I also had a couple of days where I slept for much of the day, which certainly helped.
As I believe I had a major exposure on or about January 10th, and on February 11th as I write this I am symptom-free, I hope I can consider it behind me. To my knowledge, although I am troubled by it given the transmissibility of Omicron, there is no indication that I have infected any of my family during this period.
Update complete.
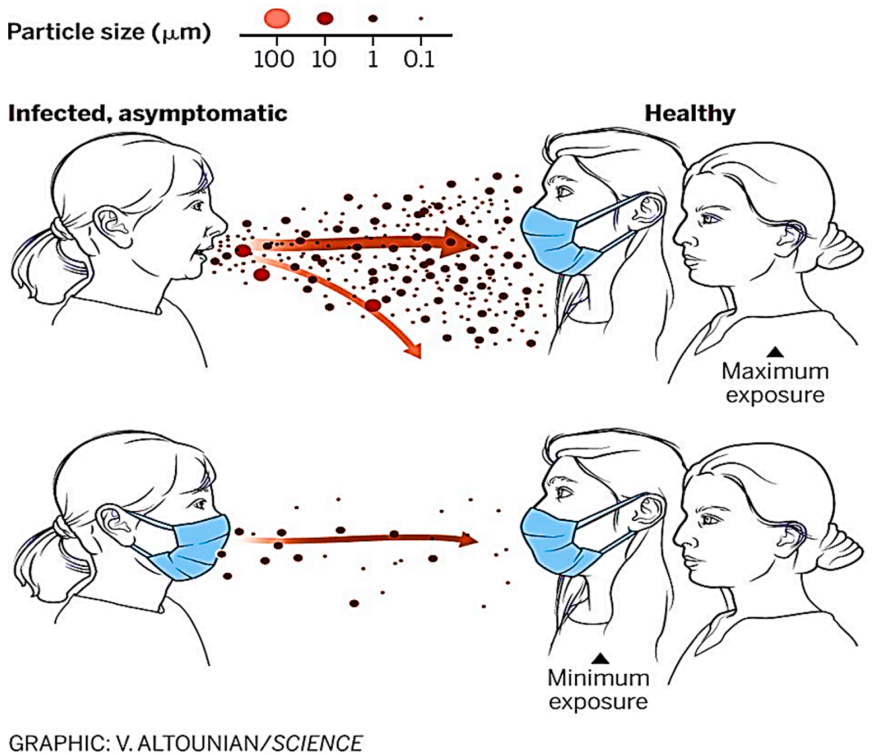
Figure 1: The Basic Principle Of The Mask For Both Infected And Non-Infected (1)
Figure 1 provides an excellent graphical explanation of the value of masking, both for the healthy and the infected. For the healthy, the mask aids in preserving one’s uninfected status – it accomplishes this via filtering, i.e. capture of incoming particles large and small. If one does become infected, it is from a relatively smaller “viral load”, where it is known that the rate of onset and seriousness of outcome is largely related to the magnitude of exposure. For the infected, the mask reduces the viral load delivered into the surrounding air or projected at another when breathing, speaking, coughing, etc. It helps protect others.
However, there is personal advantage for the infected mask wearer, this being that a mask protects the infected wearer from additional infection, i.e. incremental viral load, if exposed. This article posits that there may be a second overlooked advantage of mask wearing both for the infected and the uninfected, this owing to the impedance to air flow presented by a mask, specifically during inhalation, and what that may mean to immune function…
Personally, I have no doubt that facemasks play a vital role in the mitigation of COVID-19 transmission. Being somewhat guarded about breathing, I began exploring masks as well as air filtering technologies in 2020 at the start of the pandemic. My first question was, “What is the size of a COVID-19 virion?”, a single COVID-19 virus particle, and are masks capable of blocking that from entry or exit? As we have a HEPA plus activated carbon air filter running 24/7 in the office, I also wanted to know about it’s effectiveness in capturing COVID-19 virii. From a study conducted by the Aerosol and Bioengineering Laboratory of Konkuk University in Seoul, S.K. in 2020, the theoretical minimum size of a COVID-19 virion is .09 micron, where this “sphere” is 100% virus (1), barely small enough to pass through the pore of an N95 respirator. A spherical respiratory particle that is 1% virus and 99% other is minimally .4 micron (1). Large enough to be blocked by N95 and ASTM Levels, 3, 2, and 1 mask material.
In much of the world, masks are classified according to their ASTM Level (American Society for Testing and Materials, ASTM International). ASTM specification includes these factors: 1) Bacterial Filtration Efficiency (BFE) @ 1-5 microns, 2) Particle Filtration Efficiency (PFE) @ 0.10 micron, 3) Fluid Resistance in mmHg, and 4) Breathability – Delta Pressure in mmH2O/cm2 – this is pressure drop across the mask or effective breathing resistance experienced by the wearer. (This mask guide is a good reference.) As ASTM mask levels ascend, the filtration effectiveness and fluid resistance increase. The mask with the highest filtration rating and fluid resistance is the National Institute for Occupational Safety and Health (NIOSH) Approved N95 Respirator. It has a particle filtration efficiency of 99.9% @ 0.1 micron and is also indicated for medical use when treating patients with airborne disease. N95 masks are relatively tight, form fitting, and have a higher Breathability – Delta P, i.e. breathing is more effortful when wearing an N95 mask. The N95 mask has had this rating long before the emergence of COVID-19. It emerged in the early 1990s from research to find a mask design for health care professionals treating patients with airborne disease, e.g. tuberculosis.
ASTM and N95 masks work on the basis of “capture” and “fit”, i.e. the capture of incoming and outgoing matter, liquid and particulate, where fit is the primary weakness of all. To be form fitting, the mask must have the functional features to afford fit, i.e. metal stays, etc., and these features must be used. When a mask is not snug against the face, inhaled and exhaled air enters and exits through the gaps that exist between the face and the mask – “unfiltered”. The reality of mask wearing during COVID-19 is that most of us have not been using N95 masks but cloth masks with or without ASTM rating. Many men wear masks over copious facial hair. What advantage does this offer or has this offered during COVID times (?), primarily the capture of droplets both large and small that are normally released when speaking, coughing, sneezing, etc. This value alone has probably had a significant impact on mitigating transmission person-person and transmission via contaminated surfaces

Figure 2: Pressure Observed In The Throat At Rear Of Tongue Without Mask (Blue) Vs. With Mask (Orange), Breathing Through The Nose (Instrument: SPER Scientific Model 850097 Manometer)
But, there may be a second function at work, one that works simply on the basis of impeding inhalation, to varying degree. Here I refer to the potential for a mask to enhance the antipathogenic role of endogenous nitric oxide by increasing the amount of NO that is mixed with each inhalation – this by increasing the negative pressure exerted on the paranasal sinuses and tongue with each inhalation as a consequence of the partial blockade of air presented by the mask. A 2nd consequence of the mask may be to pressurize the paranasal sinuses and mouth/tongue cavity during exhalation, loading them with air that is then drawn out – now laden with NO – during the next inhalation. A useful way to conceive of this potential mask function is as “a nitric oxide concentrating mechanism”. It is one that our body employs all the time via the function of the nasal turbinates, shrinking and swelling in real-time to micro-mange air flow, this control being a function of nitric oxide as a signaling molecule. As a mask increases the resistance of ingoing and outgoing air flow, it adds to the function of the turbinates, presenting more negative pressure on the upper airways when inhaling and increased positive pressure on the upper airways when exhaling.
Figure 2 presents the pressure in mmH2O in the throat at the rear of the tongue without mask (blue) and with N95 mask (orange). The graphs are time independent but the cadence is approximately the same as I am breathing with RESPIRE-1 Vocal Instructive Sequence with eyes closed in each case. Pacing the breath using RESPIRE-1 facilitates equivalent diaphragm range even though the mask restricts air flow slightly. The instrument is a SPER Scientific, Model 850097 Manometer. Here I chose the N95 because it has the most impedance to air flow and a snug fit and would result in maximal negative pressure generated during inhalation. The breathability specification on the N95 is >5mmH20/square centimeter. We can see that both negative (inhalation) and positive (exhalation) pressures resulting from the N95 mask clearly exceed those of “no mask”. (Stay tuned for the same analysis with ASTM rated masks – to be published in sequential appendices.)
Per Volume 1, Issue 1, Khechari Mudra In The Time Of COVID-19, we gain this advantage mask or no mask to some degree as a function of relatively slow, deep, rhythmic breathing, i.e., the nasal turbinates throttle incoming and outgoing air flow, thereby facilitating negative pressure exerted on the paranasal sinuses and the intake of nitric oxide with each long period of inhalation, this without a forceful inhalation. One can easily see how rapid shallow breathing negates this effect. Unfortunately, this is the breathing pattern of the majority of the adult population in the developed world – to my understanding.

Figure 3: Apparatus
Two measurements were taken. First without a mask; then with a mask. Figure 3 depicts the apparatus used to make the measurement consisting of: 1) SPER manometer, 2) N95 mask, 3) clear flexible plastic tubing, 4) last few inches of hard plastic tubing. The hard plastic tubing was necessary to prevent the resting closure of the lips and teeth on the tubing from modifying the pressure reading. To make the measurement, the end of the tube was inserted between the lips and positioned such that it was centered over the rear of the tongue but extending into the throat. In the N95 case, a small slit was placed in the front of the mask to accommodate the plastic tube. With tubing in place in the mask, masking tape was used to close any opening that remained. The manometer samples and records the pressure every 2 seconds. 72 samples were recorded for each case.
Endogenous nitric oxide (NO) is being found to play a pivotal role across vertebrate life where its role in regulating vasodilation and tone has been confirmed in fish, reptiles, and mammals. We know that in humans, NO plays many roles including that of “a first line of defense” against pathogens in inhaled air. (2)
Nitric oxide is produced in the paranasal sinuses (and the tongue) where it mixes with air during both inhalation and exhalation. During inhalation it cleanses the air of pathogens that are bound for the lungs. During exhalation, NO mixes with the air that is ultimately exhaled into the external environment, NO performing the same function of policing exhaled air for pathogens, to some degree…?
The production of endogenous nitric oxide ultimately relies on nitrate that we consume in our diet. From Khechari Mudra In The Time Of COVID-19, a reference to Healthline’s “5 Ways to Increase Nitric Oxide Naturally”, regarding the importance of supplementing the diet with rich natural sources of nitrate.